What are Internal Hemorrhoids?
Painless rectal bleeding or the prolapse of anal tissue is commonly associated with symptomatic internal hemorrhoids. Prolapse occurs when hemorrhoidal tissue from inside the anal canal comes out during a bowel movement or when wiping. This tissue often returns inside the anus on its own, or it can be gently pushed back in by the patient. Symptoms usually develop slowly over time and are often intermittent.
Classification of Internal Hemorrhoids
Internal hemorrhoids are graded based on the degree of prolapse, which helps guide treatment:
- Grade 1: No prolapse
- Grade 2: Prolapse that returns inside on its own
- Grade 3: Prolapse that must be pushed back in by the patient
- Grade 4: Prolapse that cannot be pushed back in (often painful)
Common Symptoms
Bleeding from internal hemorrhoids is typically bright red and may appear on toilet paper, drip into the toilet bowl, or be streaked on the stool. Not every patient experiences significant bleeding—some may have prolapse as their primary or only symptom. Prolapsing tissue can cause:
- Irritation or itching around the anus
- Mucus discharge
- Difficulty cleaning after a bowel movement
- A sensation that stool is “stuck” at the anus Patients who have internal hemorrhoids without symptoms do not require treatment.
What Causes Symptomatic Hemorrhoids?
Most factors linked to hemorrhoidal symptoms involve increased abdominal pressure that is transmitted to the anal region. These include:
- Straining during bowel movements
- Constipation
- Diarrhoea
- Pregnancy
- Irregular bowel habits
Examination
After reviewing your symptoms and personal and family medical history, your doctor will perform an office examination. This typically includes:
- Visual inspection of the anal area
- Digital rectal exam (placing a gloved finger into the rectum)
- Anoscopy, where a small, finger-sized instrument is inserted into the anus to directly view the hemorrhoidal tissue
- Flexible sigmoidoscopy views the lower half of the colon
- Colonoscopy usually allows visualization of the entire colon
Non-Surgical Treatment of Internal Hemorrhoids
A wide range of treatments are available for symptomatic internal hemorrhoids. The appropriate approach depends on the grade of the hemorrhoids and the severity of symptoms. Many patients improve with dietary and lifestyle modifications alone. If symptoms fail to respond, or if they are severe at the outset, office-based or surgical procedures may be recommended.
-
1. Dietary & Lifestyle Changes
- Normalizing bowel function
- Avoiding straining
- Preventing both hard stools and diarrhea
-
Fiber Intake
- 20–35 grams of fiber per day from food (fruits, vegetables, whole grains)
- Daily fiber supplement (1–2 times per day), available as powders, chewables, or capsules
-
Hydration
- 8–10 glasses of fluid daily
-
Bowel Habits
- Avoid straining
- Avoid prolonged time on the toilet
- Respond promptly to the urge to defecate (do not suppress repeatedly)
-
Exercise
-
2. Medical Treatment
- Hydrocortisone (anti-inflammatory)
- Phenylephrine (vasoconstrictor)
- Pramoxine(anesthetic)
- Witch hazel (astringent)
-
3. Phlebotonics
- Plant-based flavonoids
- Synthetic compounds (e.g., calcium dobesilate)
Office-Based Treatment for Internal Hemorrhoids
Several effective office-based therapies exist for treating internal hemorrhoids. These procedures are not designed for external hemorrhoids and are typically used when dietary and lifestyle changes do not provide enough relief. The most commonly performed procedures are:
- Rubber Band Ligation (RBL)
- Injection Sclerotherapy
- Infrared Coagulation (IRC) These options are best suited for Grade I–II and some Grade III internal hemorrhoids.
Internal Hemorrhoid Options
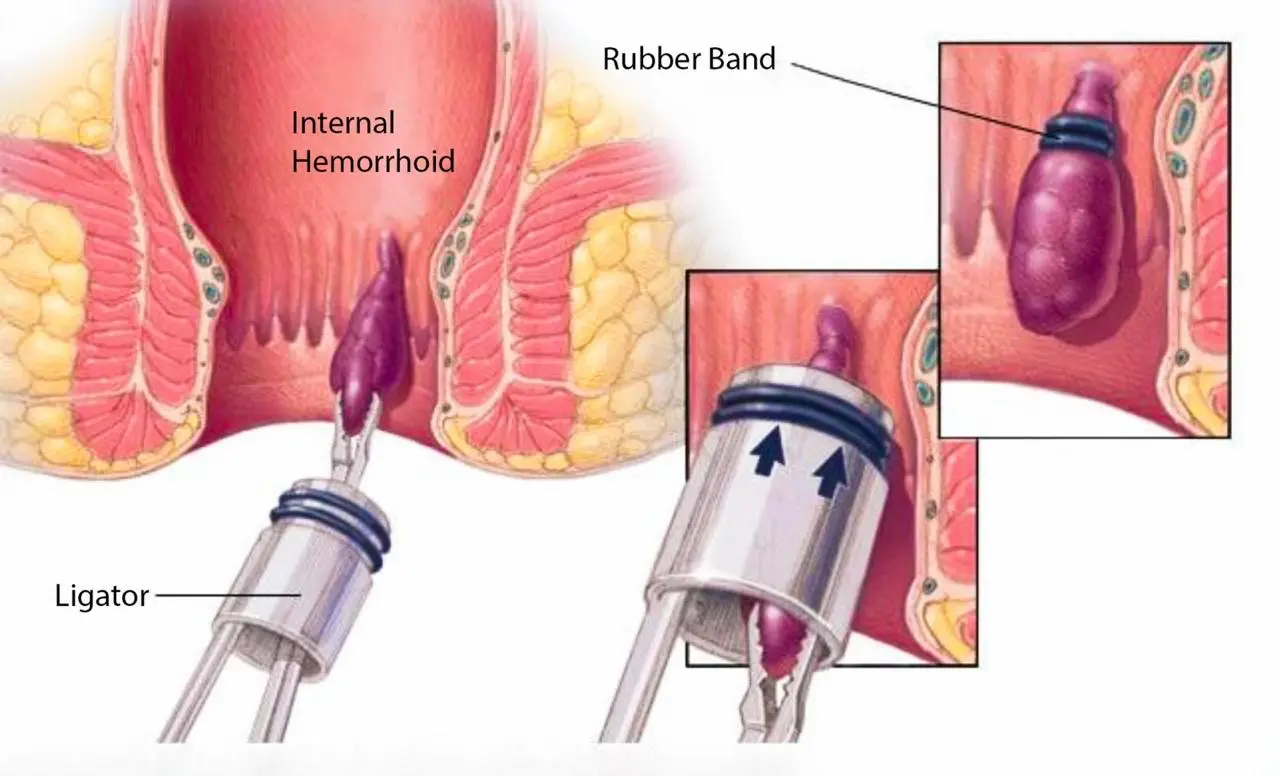
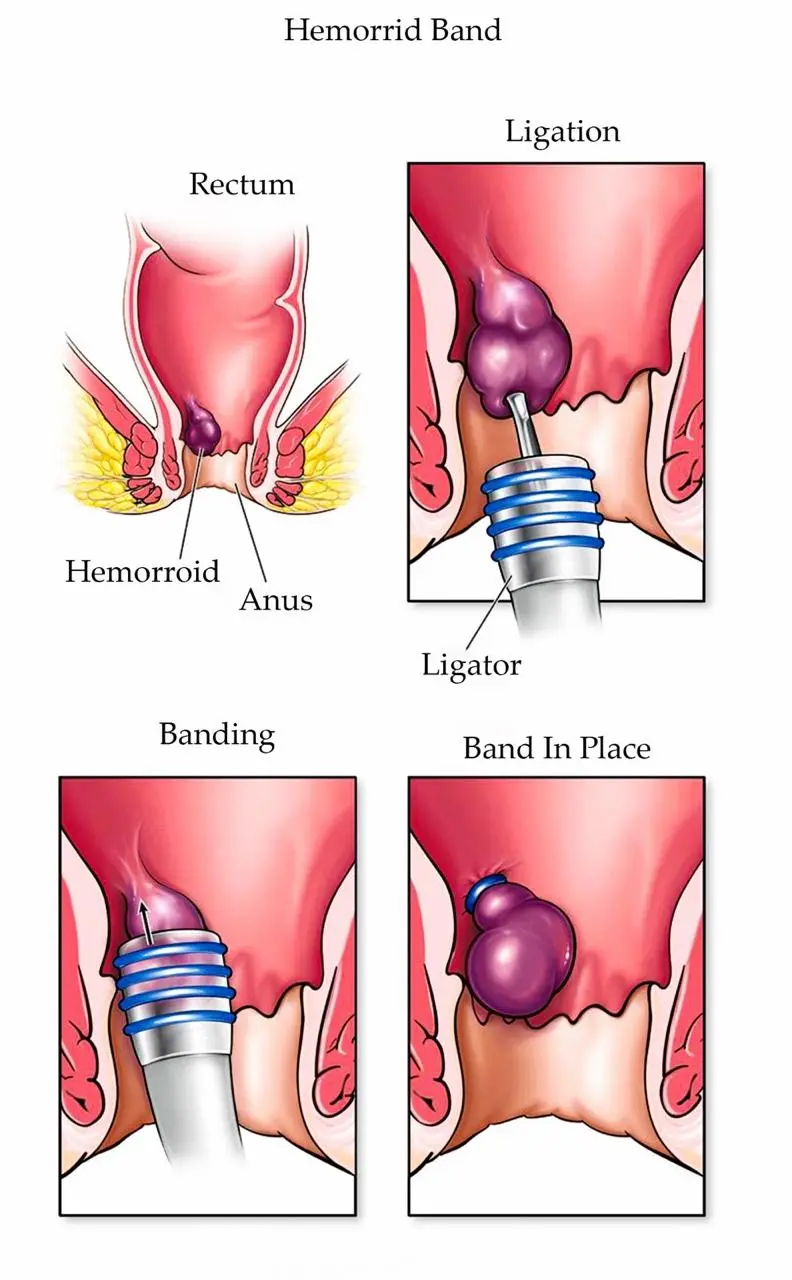
Rubber Band Ligation (RBL)
Rubber band ligation is considered the most effective office-based treatment for internal hemorrhoids. It is commonly used for:
- Grade I and II internal hemorrhoids
- Selected Grade III hemorrhoids that do not respond to conservative measures
- Cuts off blood supply to the hemorrhoid
- Causes the tissue to slough off within 1–10 days
- Promotes fixation of mucosa to submucosa, improving prolapse
- Patients on blood thinners such as warfarin, heparin, or clopidogrel may not be candidates
- Typically 1–2 bands can be placed per session
- Multiple sessions may be required
- Most patients have no significant downtime
- A mild pressure or ache for 1–3 days is common and usually relieved by acetaminophen
- Symptom improvement is often long-lasting if dietary and lifestyle changes continue
Elastic Band Ligation
If symptoms recur, repeat RBL can be performed. Surgical hemorrhoidectomy remains an option for refractory cases. Safety & Complications RBL has been shown to have:
- Lower complication rates
- Lower cost
- Similar or improved outcomes compared to excisional hemorrhoidectomy or hemorrhoid artery ligation
- Pain
- Bleeding
- Infection
- Fever
- Severe anal pain
- Urinary difficulty
- Fecal incontinence
- Nausea/vomiting
Injection Sclerotherapy
Sclerotherapy involves injecting a sclerosing agent into the hemorrhoidal tissue to produce:
- Inflammation
- Fibrosis
- Scar fixation of mucosa to submucosa
- Quick and often painless
- May require multiple short sessions
- Can be considered in some patients on anticoagulants, depending on clinical judgment
- Post-procedure pain: 24%–49%
- Post-procedure bleeding: 0.9%–6%
- Recurrent bleeding: 1.5%–29%
- Recurrent prolapse: ~16%
Infrared Coagulation (IRC)
Infrared coagulation is another office-based option for:
- Grade I
- Grade II
- Selected Grade III internal hemorrhoids
- A small probe delivers infrared radiation
- The tissue heats, becomes inflamed, sloughs, and scars
- This reduces excess prolapsing tissue
- Quick and generally well tolerated
- Few complications
- Multiple treatments may be required
- Post-procedure pain: 16%–100%
- Post-procedure bleeding: 15%–44%
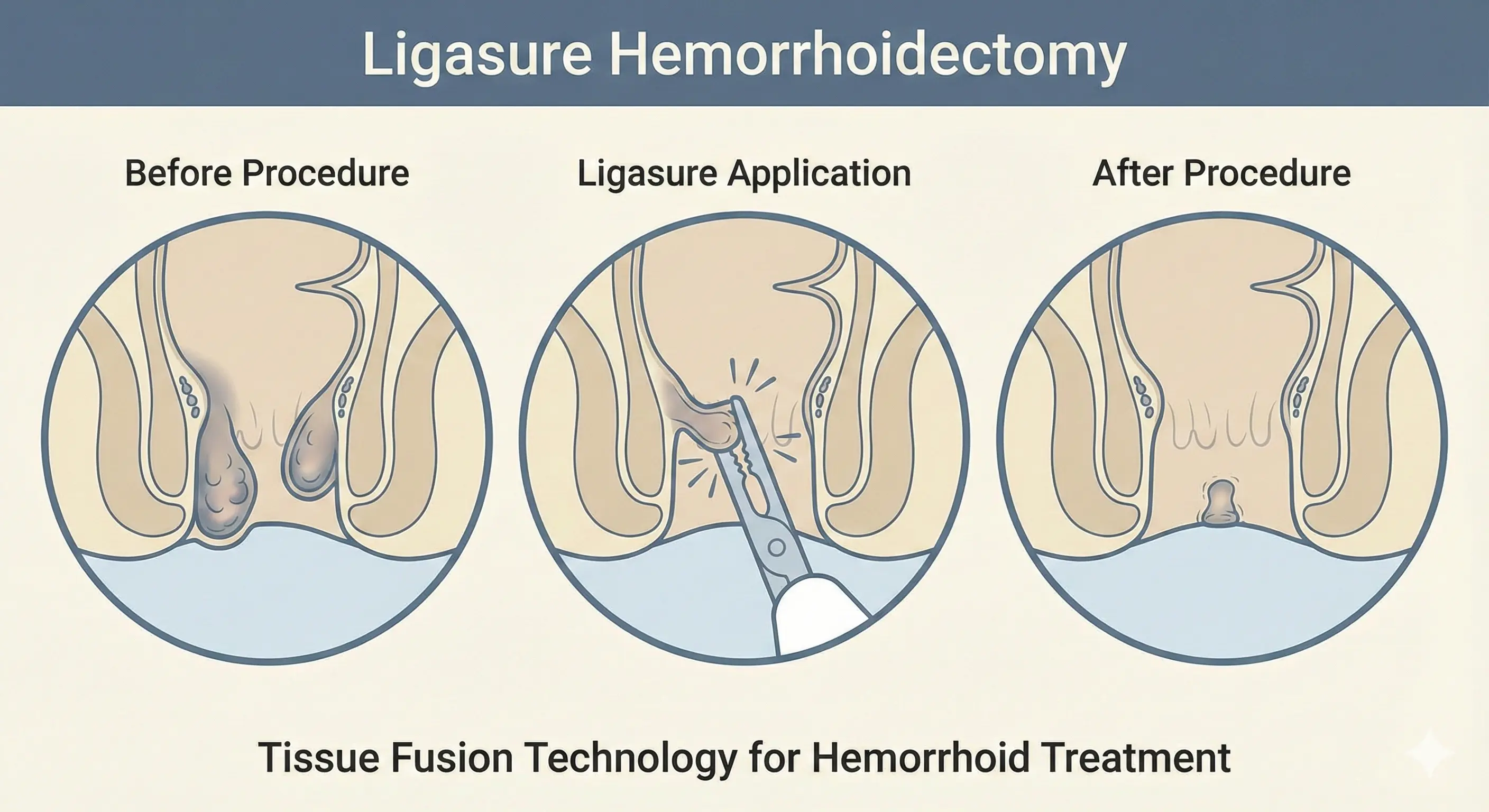
Excisional Hemorrhoidectomy
- Excisional Hemorrhoidectomy (EH), or surgical removal of hemorrhoidal tissue, is
typically offered to select patients with external hemorrhoids or symptomatic combined
internal and external hemorrhoids (grades III–IV). It remains an effective option for
patients who fail, cannot tolerate, or are not candidates for office-based procedures, or for
those with significant external disease.
-
Both open and closed excisional hemorrhoidectomy techniques may be used, and surgery
can be performed with a variety of surgical devices.
- Hemorrhoidectomy is performed in an operating room and may be done under sedation, general anesthesia, or spinal anesthesia (similar to an epidural during childbirth).
- Serious complications after surgical hemorrhoidectomy are rare. The most common complication is postoperative hemorrhage. Acute urinary retention occurs in approximately 1% to 15% of cases and is the most frequent cause of delayed discharge in ambulatory settings. Long-term complications may include anal stricture and fecal incontinence.
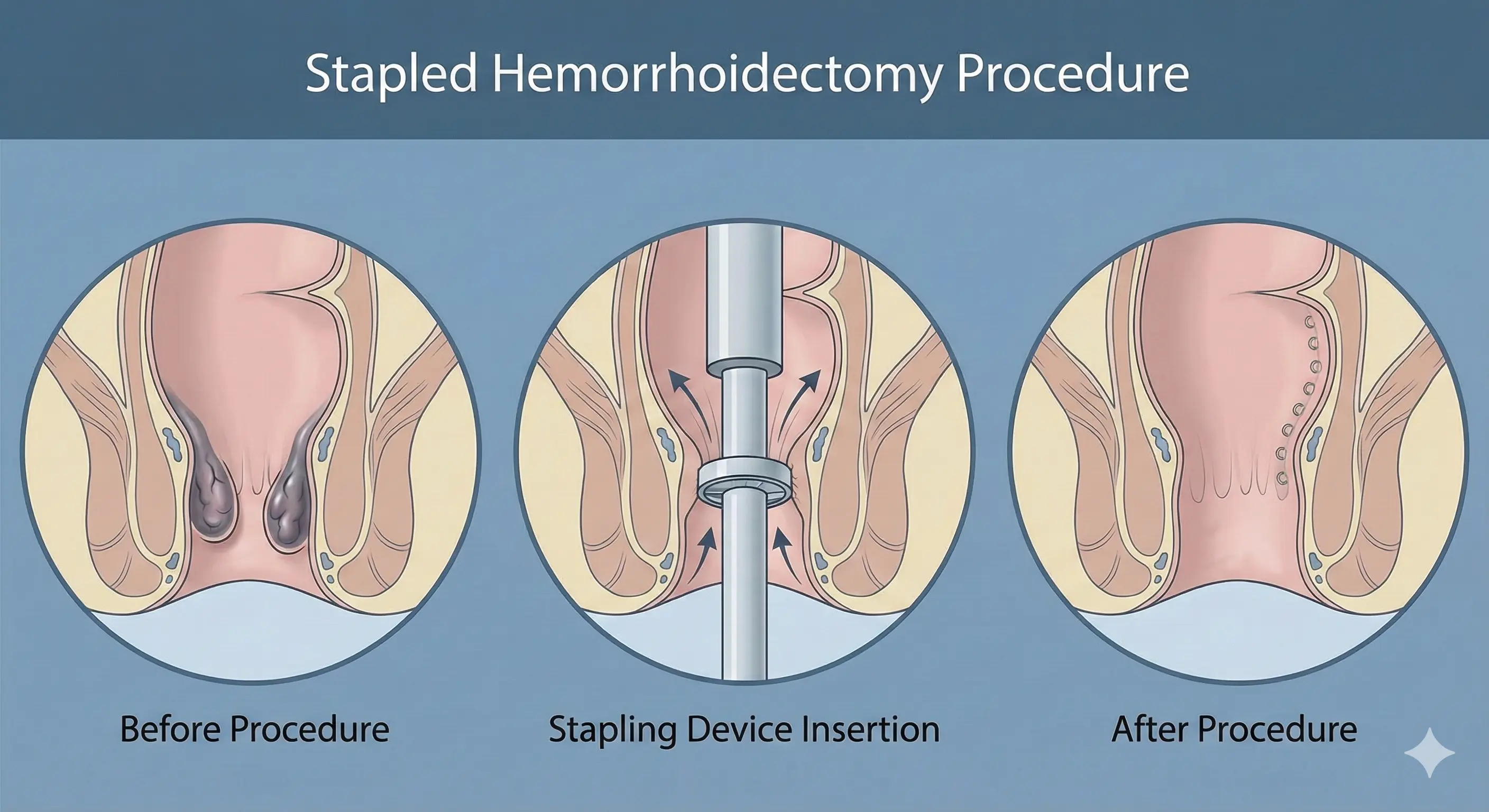
Stapled Hemorrhoidectomy
-
Stapled hemorrhoidopexy is not routinely recommended as a first-line surgical
treatment for internal hemorrhoids due to its marginal efficacy and significant risk
profile.
- SH employs a circular stapling device to excise a ring of submucosa proximal to the dentate line, creating a mucosa-to-mucosa anastomosis that elevates the anal cushions and interrupts feeding vessels. Although effective for prolapsing internal hemorrhoids, it does not address external hemorrhoids.
- SH is also associated with several unique complications, including rectovaginal fistulas, staple line bleeding, and staple line strictures.
Doppler-Guided Hemorrhoidal Artery Ligation (HAL)
-
Doppler-guided hemorrhoidal artery ligation may be used for patients with internal
hemorrhoids. HAL uses an anoscope equipped with a Doppler probe to identify
hemorrhoidal arteries, allowing for targeted suture ligation. Advantages include the
absence of tissue excision and potentially less postoperative pain. It may also be
combined with mucopexy for symptomatic hemorrhoidal prolapse.
- However, compared with rubber band ligation (RBL), patients typically experience more pain in the early postoperative period following HAL. HAL is also more expensive and has demonstrated reduced cost-effectiveness compared with RBL.
Postoperative Instructions After Hemorrhoidectomy
- Pain Management:
Some pain is expected after hemorrhoid surgery. The goal is to keep it manageable.
Full activity may take 2–4 weeks to resume. Pain medication is usually a combination of
narcotic and non-narcotic medicines. We aim to limit the use of stronger narcotics to
reduce side effects.
- Try urinating while sitting in a sitz bath.
- If unsuccessful, contact the surgeon’s office or go to the emergency department for bladder catheterization. Failure to address this can cause permanent bladder damage from over- stretching.
- Follow a high-fiber diet.
- Take a fiber supplement.
- Drink plenty of liquids.
-
Sitz Baths:
Sitting in a warm bath (sitz bath) 2–3 times per day for 10–15 minutes can provide
significant relief.
Urination Issues:
Occasionally, patients may have difficulty urinating after surgery. If this happens:
Book Your Appointment
Select a Doctor
Select Date & Time
Select a Branch
Scottsdale
Click to select this branch
Peoria
Click to select this branch